SCN5A/Nav1.5,电压门控钠通道5α抗体
产品名称: SCN5A/Nav1.5,电压门控钠通道5α抗体
英文名称: Anti-SCN5A/Nav1.5 antibody
产品编号: HZ-9445R
产品价格: null
产品产地: 中国/美国
品牌商标: HZbscience
更新时间: 2023-08-17T10:24:20
使用范围: WB,ELISA,IHC-P,IHC-F,IF
- 联系人 : 鲍丽雯
- 地址 : 上海市闵行区闵北路88弄1-30号第22幢AQ136室
- 邮编 : 200612
- 所在区域 : 上海
- 电话 : 139****0749
- 传真 : 021-60345367
- 邮箱 : www.shzbio.net
SCN5A/Nav1.5,电压门控钠通道5α抗体
产品编号HZ-9445R
英文名称SCN5A/Nav1.5
中文名称电压门控钠通道5α抗体
别 名Cardiac tetrodotoxin insensitive voltage dependent sodium channel alpha subunit; CDCD2; CMD1E; CMPD2; HB1; HB2; HBBD; HH1; ICCD; IVF; LQT3; PFHB1; Scn5a (gene name); Scn5a; SCN5A_HUMAN; Sodium channel protein cardiac muscle alpha subunit; Sodium channel protein cardiac muscle alpha-subunit; Sodium channel protein cardiac muscle subunit alpha; Sodium channel protein type 5 subunit alpha; Sodium channel protein type V alpha subunit; Sodium channel protein type V subunit alpha; SSS1; VF1; Voltage gated sodium channel alpha subunit Nav1.5; Voltage-gated sodium channel alpha subunit Nav1.5; Voltage-gated sodium channel subunit alpha Nav1.5.
说 明 书0.1ml 0.2ml
研究领域
抗体来源Rabbit
克隆类型Polyclonal
交叉反应 Human, Mouse, Rat, Chicken, Dog, Pig, Horse, Rabbit, Zebrafish, Sheep, Chimpanzee, mpanzee,
SCN5A/Nav1.5,电压门控钠通道5α抗体产品应用ELISA=1:500-1000 IHC-P=1:100-500 IHC-F=1:100-500 IF=1:50-200 (石蜡切片需做抗原修复)
not yet tested in other applications.
optimal dilutions/concentrations should be determined by the end user.
分 子 量227kDa
细胞定位细胞膜
性 状Lyophilized or Liquid
浓 度1mg/1ml
免 疫 原KLH conjugated synthetic peptide derived from human Nav1.5/SCN5A
亚 型IgG
纯化方法affinity purified by Protein A
储 存 液0.01M TBS(pH7.4) with 1% BSA, 0.03% Proclin300 and 50% Glycerol.
保存条件Store at -20 °C for one year. Avoid repeated freeze/thaw cycles. The lyophilized antibody is stable at room temperature for at least one month and for greater than a year when kept at -20°C. When reconstituted in sterile pH 7.4 0.01M PBS or diluent of antibody the antibody is stable for at least two weeks at 2-4 °C.
SCN5A/Nav1.5,电压门控钠通道5α抗体PubMedPubMed
产品介绍background:
This protein mediates the voltage-dependent sodium ion permeability of excitable membranes. Assuming opened or closed conformations in response to the voltage difference across the membrane, the protein forms a sodium-selective channel through which Na(+) ions may pass in accordance with their electrochemical gradient. It is a tetrodotoxin-resistant Na(+) channel isoform. This channel is responsible for the initial upstroke of the action potential.
Function:
This protein mediates the voltage-dependent sodium ion permeability of excitable membranes. Assuming opened or closed conformations in response to the voltage difference across the membrane, the protein forms a sodium-selective channel through which Na(+) ions may pass in accordance with their electrochemical gradient. It is a tetrodotoxin-resistant Na(+) channel isoform. This channel is responsible for the initial upstroke of the action potential. Channel inactivation is regulated by intracellular calcium levels.
Subunit:
Interacts with the PDZ domain of the syntrophin SNTA1, SNTB1 and SNTB2 (By similarity). Interacts with NEDD4, NEDD4L, WWP2 and GPD1L. Interacts with CALM. Interacts with FGF13; the interaction is direct and may regulate SNC5A density at membranes and function.
Subcellular Location:
Membrane.
SCN5A/Nav1.5,电压门控钠通道5α抗体Tissue Specificity:
Found in jejunal circular smooth muscle cells (at protein level). Expressed in human atrial and ventricular cardiac muscle but not in adult skeletal muscle, brain, myometrium, liver, or spleen. Isoform 4 is expressed in brain.
Post-translational modifications:
Regulated through phosphorylation by CaMK2D (By similarity).
Ubiquitinated by NEDD4L; which promotes its endocytosis. Does not seem to be ubiquitinated by NEDD4 or WWP2.
DISEASE:
Defects in SCN5A are a cause of progressive familial heart block type 1A (PFHB1A) [MIM:113900]; also known as Lenegre-Lev disease or progressive cardiac conduction defect (PCCD). PFHB1A is an autosomal dominant cardiac bundle branch disorder that may progress to complete heart block. PFHB1A is characterized by progressive alteration of cardiac conduction through the His-Purkinje system with right or left bundle branch block and widening of QRS complexes, leading to complete atrioventricular block and causing syncope and sudden death. [DISEASE] Defects in SCN5A are the cause of long QT syndrome type 3 (LQT3) [MIM:603830]. Long QT syndromes are heart disorders characterized by a prolonged QT interval on the ECG and polymorphic ventricular arrhythmias. They cause syncope and sudden death in response to exercise or emotional stress. LQT3 inheritance is an autosomal dominant.
Defects in SCN5A are the cause of Brugada syndrome type 1 (BRGDA1) [MIM:601144]. An autosomal dominant tachyarrhythmia characterized by right bundle branch block and ST segment elevation on an electrocardiogram (ECG). It can cause the ventricles to beat so fast that the blood is prevented from circulating efficiently in the body. When this situation occurs (called ventricular fibrillation), the individual will faint and may die in a few minutes if the heart is not reset.
Defects in SCN5A are the cause of sick sinus syndrome type 1 (SSS1) [MIM:608567]. The term 'sick sinus syndrome' encompasses a variety of conditions caused by sinus node dysfunction. The most common clinical manifestations are syncope, presyncope, dizziness, and fatigue. Electrocardiogram typically shows sinus bradycardia, sinus arrest, and/or sinoatrial block. Episodes of atrial tachycardias coexisting with sinus bradycardia ('tachycardia-bradycardia syndrome') are also common in this disorder. SSS occurs most often in the elderly associated with underlying heart disease or previous cardiac surgery, but can also occur in the fetus, infant, or child without heart disease or other contributing factors, in which case it is considered to be a congenital disorder.
Defects in SCN5A are the cause of familial paroxysmal ventricular fibrillation type 1 (VF1) [MIM:603829]. A cardiac arrhythmia marked by fibrillary contractions of the ventricular muscle due to rapid repetitive excitation of myocardial fibers without coordinated contraction of the ventricle and by absence of atrial activity.
Defects in SCN5A may be a cause of sudden infant death syndrome (SIDS) [MIM:272120]. SIDS is the sudden death of an infant younger than 1 year that remains unexplained after a thorough case investigation, including performance of a complete autopsy, examination of the death scene, and review of clinical history. Pathophysiologic mechanisms for SIDS may include respiratory dysfunction, cardiac dysrhythmias, cardiorespiratory instability, and inborn errors of metabolism, but definitive pathogenic mechanisms precipitating an infant sudden death remain elusive. Long QT syndromes-associated mutations can be responsible for some of SIDS cases.
SCN5A/Nav1.5,电压门控钠通道5α抗体Defects in SCN5A may be a cause of familial atrial standstill (FAS) [MIM:108770]. Atrial standstill is an extremely rare arrhythmia, characterized by the absence of electrical and mechanical activity in the atria. Electrocardiographically, it is characterized by bradycardia, the absence of P waves, and a junctional narrow complex escape rhythm.
Defects in SCN5A are the cause of cardiomyopathy dilated type 1E (CMD1E) [MIM:601154]; also known as dilated cardiomyopathy with conduction disorder and arrhythmia or dilated cardiomyopathy with conduction defect 2. Dilated cardiomyopathy is a disorder characterized by ventricular dilation and impaired systolic function, resulting in congestive heart failure and arrhythmia. Patients are at risk of premature death.
Defects in SCN5A are the cause of familial atrial fibrillation type 10 (ATFB10) [MIM:614022]. ATFB10 is a familial form of atrial fibrillation, a common sustained cardiac rhythm disturbance. Atrial fibrillation is characterized by disorganized atrial electrical activity and ineffective atrial contraction promoting blood stasis in the atria and reduces ventricular filling. It can result in palpitations, syncope, thromboembolic stroke, and congestive heart failure.
Similarity:
Belongs to the sodium channel (TC 1.A.1.10) family. Nav1.5/SCN5A subfamily.
Contains 1 IQ domain.
Gene ID:
6331
Database links:
Entrez Gene: 6331 Human
Omim: 600163 Human
SwissProt: Q14524 Human
Unigene: 517898 Human
Important Note:
This product as supplied is intended for research use only, not for use in human, therapeutic or diagnostic applications.
SCN5A/Nav1.5,电压门控钠通道5α抗体Involvement in disease;Defects in SCN5A are a cause of progressive familial heart block type 1A (PFHB1A); also known as Lenegre-Lev disease or progressive cardiac conduction defect (PCCD). PFHB1A is an autosomal dominant cardiac bundle branch disorder that may progress to complete heart block. PFHB1A is characterized by progressive alteration of cardiac conduction through the His-Purkinje system with right or left bundle branch block and widening of QRS complexes, leading to complete atrio-ventricular block and causing syncope and sudden death.
Defects in SCN5A are the cause of long QT syndrome type 3 (LQT3). Long QT syndromes are heart disorders characterized by a prolonged QT interval on the ECG and polymorphic ventricular arrhythmias. They cause syncope and sudden death in response to exercise or emotional stress. LQT3 inheritance is an autosomal dominant.
Defects in SCN5A are the cause of Brugada syndrome type 1 (BRS1). BRS1 is an autosomal dominant tachyarrhythmia characterized by right bundle branch block and ST segment elevation on an electrocardiogram (ECG). It can cause the ventricles to beat so fast that the blood is prevented from circulating efficiently in the body. When this situation occurs (called ventricular fibrillation), the individual will faint and may die in a few minutes if the heart is not reset.
| 产品图片 | 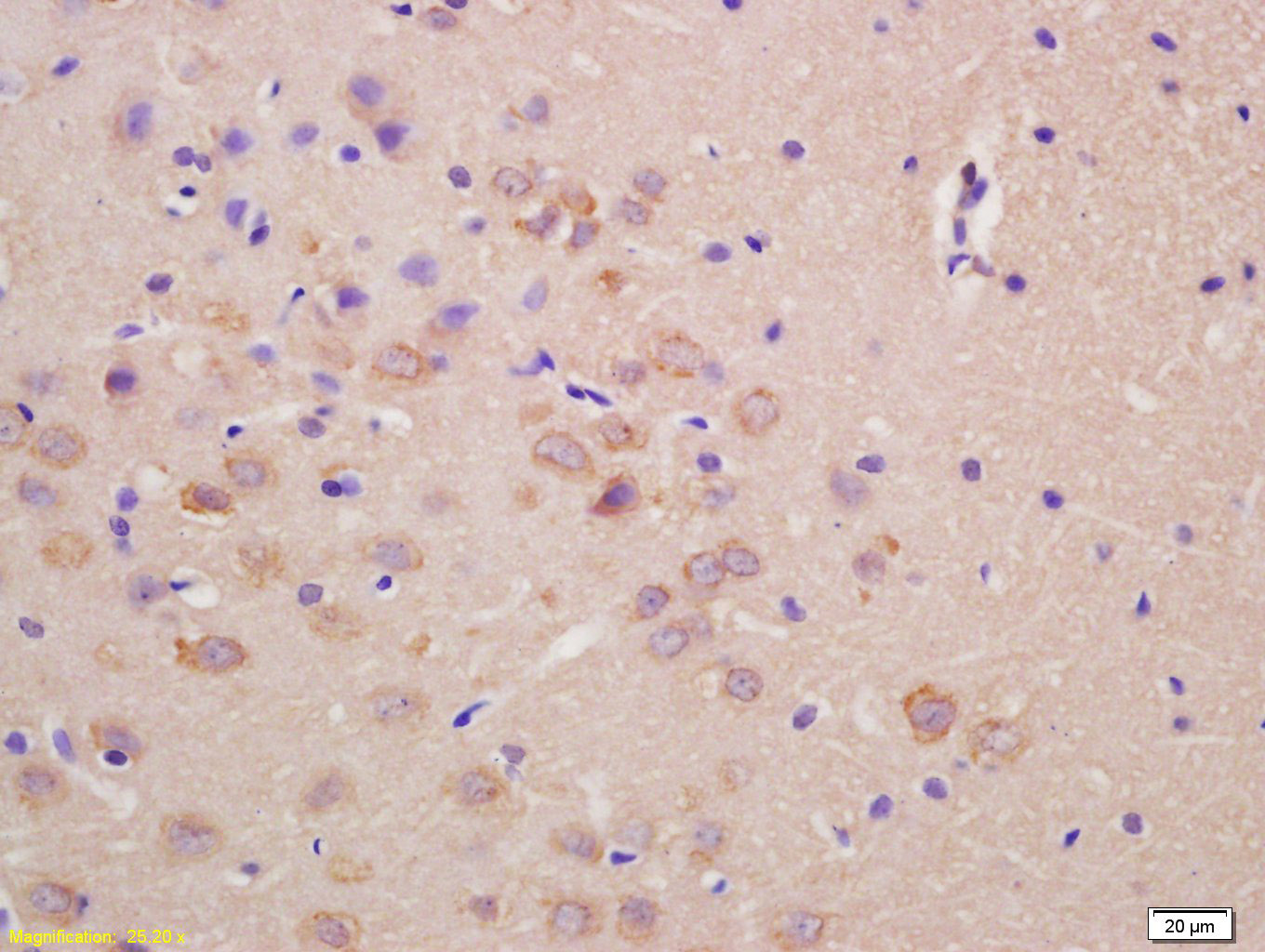
Tissue/cell: rat brain tissue; 4% Paraformaldehyde-fixed and paraffin-embedded;
Antigen retrieval: citrate buffer ( 0.01M, pH 6.0 ), Boiling bathing for 15min; Block endogenous peroxidase by 3% Hydrogen peroxide for 30min; Blocking buffer (normal goat serum,C-0005) at 37℃ for 20 min; Incubation: Anti-SCN5A Polyclonal Antibody, Unconjugated(HZ-9445R) 1:200, overnight at 4°C, followed by conjugation to the secondary antibody(SP-0023) and DAB(C-0010) staining 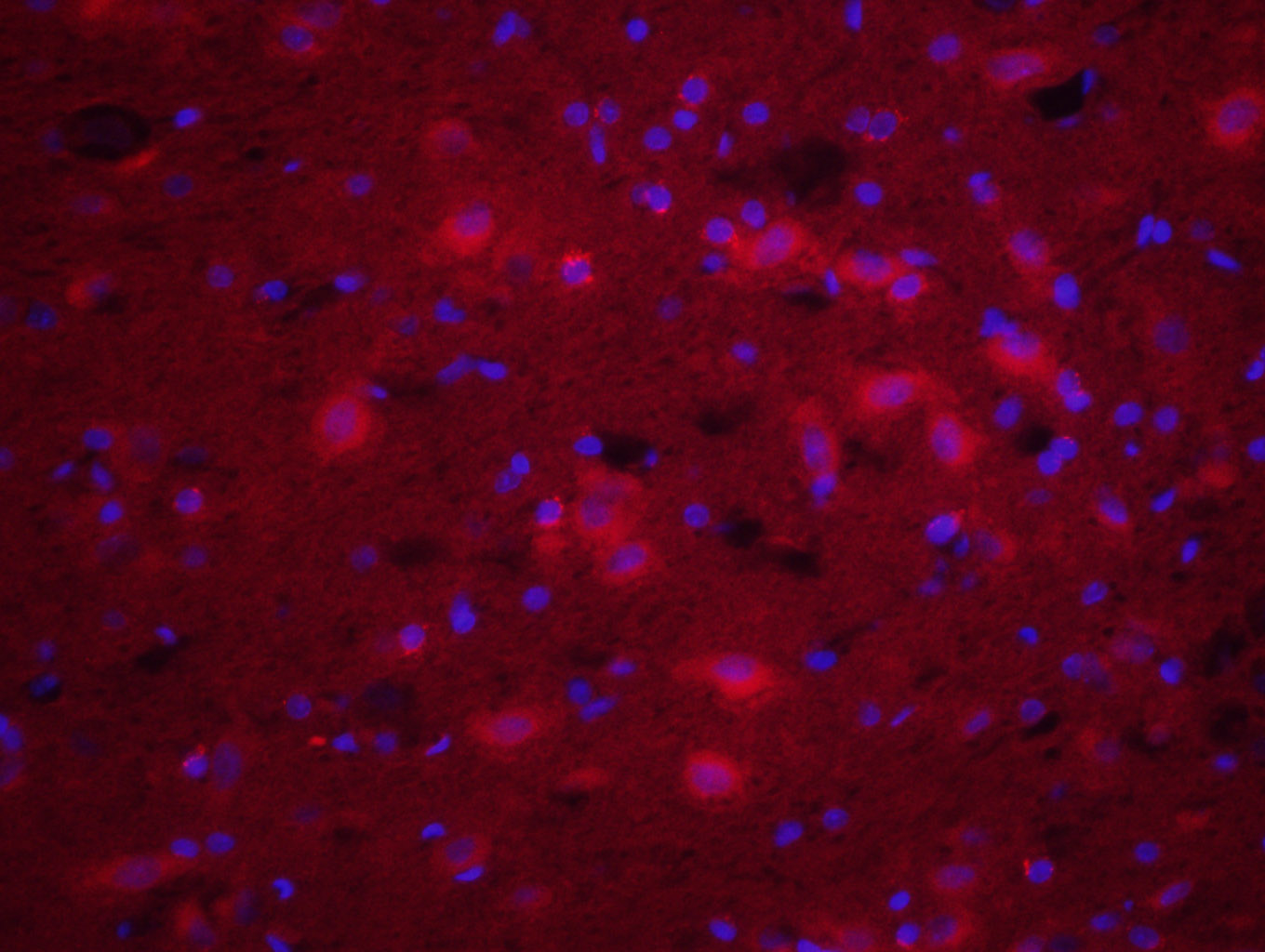
Tissue/cell: rat brain tissue;4% Paraformaldehyde-fixed and paraffin-embedded;
Antigen retrieval: citrate buffer ( 0.01M, pH 6.0 ), Boiling bathing for 15min; Blocking buffer (normal goat serum,C-0005) at 37℃ for 20 min; Incubation: Anti-SCN5A Polyclonal Antibody, Unconjugated(HZ-9445R) 1:200, overnight at 4°C; The secondary antibody was Goat Anti-Rabbit IgG, Cy3 conjugated(HZ-0295G-Cy3)used at 1:200 dilution for 40 minutes at 37°C. DAPI(5ug/ml,blue,C-0033) was used to stain the cell nuclei |